-

Cycadia 3301
Telephone & Hampshire Lodge No. 3301 is a London-based Masonic lodge operating under the United Grand Lodge of England, established in 1908 by employees of the National Telephone Company. It is a recognized, traditional occupational lodge with a rich history of, particularly during WW2. The trial had previously heard Connolly…
-

CHARGES BOUGHT
In the Tapas group (the friends dining with the McCanns on May 3, 2007), at least five were qualified medical doctors (some sources list four who trained together at Leicester University, but statements confirm five practicing or qualified): Gerry McCann (cardiologist) Kate McCann (former GP/anaesthetist)David Payne (cardiovascular consultant/researcher) Fiona Payne…
-
Father Jose Manuel Pacheco
Conceicao Calado Pacheco TRANSLATIONS BY INES13- Processo Vol XIII 3924 to 392613_VOLUME_XIIIa_Page_392413_VOLUME_XIIIa_Page_392513_VOLUME_XIIIa_Page_3926 Translation of Father Pachecos Statement to the PJ 30th October 2007 Jose Manuel Conceicao Pacheco The first time he had contact with the McCann’s was on 5th May at about 19.00. This was a personal contact with them…
-
Rachel Oldfield
OFFICIAL INQUIRY FILES and DOCUMENTSRACHAEL OLDFIELD’S STATEMENTSitemap This information belongs to the Ministério Público in Portimão, Portugal. It was released to the public on 4 August 2008 in accordance with Portuguese LawRachael Oldfield’s statement 04/05/07 @ 19.2073 to 76 Witness statement of Rachel Mariamma Jean Mampilly 2007.05.04TRANSLATION BY ANNA/ALBYM01-Processo 01-…
-

Fiona Payne
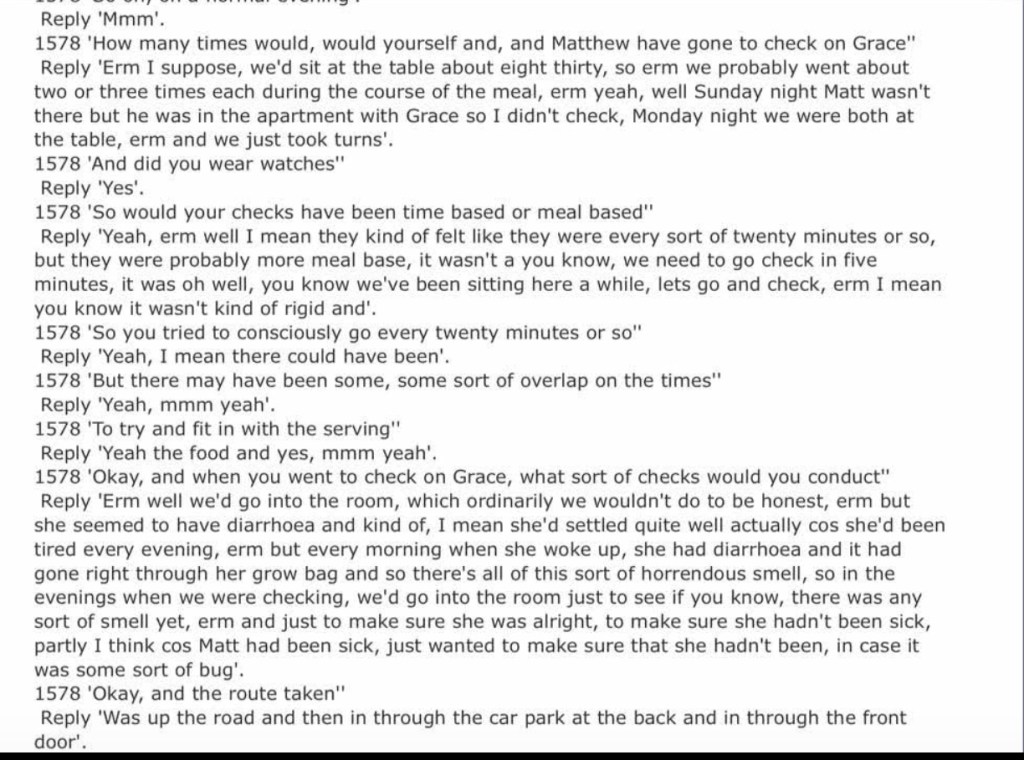
Excerpt from Fiona Payne’s Rogatory Interview (10.4.08)1485 – “What were the circumstances regarding her telling you that?” Reply – “She did, she brought it up and that she, I mean, this is awful in retrospect as well, she asked what my opinion was on, erm, tut, on whether they were…
-

Veterans Introduction to Ai
Once an Illuminating Knight, Always an illuminating Knight Intro to Ai What is ai Ai works best as a digital note pad in any field taking your thoughts and ideas enchancing and documenting with less effort on your part Be that excell, word, or just notes on recipes ai can…
-

Priori Du Sion Recruitment
Priori sion recruitment structure Illuminate corruption crime and points of issue within your local community Ensure 10/10 maths 3 point proof external validation and no cherry picking Email /call/post to 3+ agency ensure cross state/city jurisdiction Include dates, times, names, positions registrations addresses and legal statute broken Use an ai…


-
Subscribe
Subscribed
Already have a WordPress.com account? Log in now.
